
Last Updated on June 10, 2019 by
 Heart surgery is everywhere. Most Americans – 70% – contract heart disease. It’s the leading cause of death, even ahead of cancer.
Heart surgery is everywhere. Most Americans – 70% – contract heart disease. It’s the leading cause of death, even ahead of cancer.
Three months ago I had sudden heart surgery to replace my mitral valve, and that’s the only reason I’m here with you today. This blog describes my experience, in hopes that it will help you better watch your own health, and better deal with any heart problems that you encounter. I also hope that this blog about emergency surgery will help you toward surgery success if you face a similar emergency.
How it happened: In late October I visited my cardiologist Dr Sarine John-Rosman for a routine checkup. She talked with me, ran some tests, and immediately popped me into the hospital.
I was doubly lucky. I was lucky that Dr John had a keen diagnostic sense, even though I lacked most symptoms of my disease, endocarditis. Her alertness probably saved my life. And I was lucky that my recovery from heart surgery proceeded so well that later on the cardio team complained that I was a “boring patient” to visit.
More Than You Wanted to Know About Elephants
As I remarked once before, my friend Jim Blue used to say, “It’s like the book about elephants – it tells you more than you ever wanted to know about elephants.” Today, we call this Too Much Information.
If you find this blog TMI about heart surgery, well, I forgive you. Feel free to skip forward to portions of interest. However, if you at least skim it, I believe you will be better equipped to keep an eye on that essential organ, your heart.
This blog is in five parts, which will appear over the next few weeks:
1: Heart Surgery – Highly Likely for You or a Family Member
2: What Brings Us to the Operating Room Before Surgery
3: Valve Surgery Operation and the Intensive Care Unit
4: Life Beyond: Post Surgery Recovery
5: Heart Surgery Cost – Medicare Coverage and Hospital Staff
Today’s installment is not too scary. Similarly, parts 2 and 5. Parts 3 and 4 go into detail about heart surgery, which might upset the squeamish. However, it’s all stuff that you might find useful to know.
I can say, now that I’ve survived the experience, I’m not as squeamish as I used to be!
Why You Should Care About Heart Problems
My particular heart disease was a low probability event. Therefore, why should you as a reader care about my adventure with it?
There are some excellent reasons why you should care:
 1. You Will Probably Contract Cardiovascular Disease (CVD): 70% of Americans age 60 and older have cardiovascular disease (CVD).(see Heart Disease and Stroke Statistics—2013 Update, chart 13-1)
1. You Will Probably Contract Cardiovascular Disease (CVD): 70% of Americans age 60 and older have cardiovascular disease (CVD).(see Heart Disease and Stroke Statistics—2013 Update, chart 13-1)
2. Heart Disease Is Very Likely To Kill You: If you’re a typical American, you’re more likely to die from heart disease than any other cause. Cancer is a close second, but every other cause is much much less probable.
3. Surgery Is Likely: Heart surgery is a high probability need when you contract heart disease. Lifestyle changes and medications are clearly not enough for most people, because heart disease claims so many deaths. Surgery is the next and only remaining treatment option.
4. It’s Very Serious: Every kind of heart disease and heart surgery is serious. It is literally a matter of life and death.
Be Ready For Anything:
Heart surgery comes in many forms. Here are some of the most common types in rough order of complexity:
– Irregular Heart Beat:
Arrhythmia, when not controlled by drugs, requires surgery to install a pacemaker or an implantable cardioverter-defibrillator (ICD).
– Aneurysm:
A bulge in the heart wall or in a nearby blood vessel that could kill if it ruptures. A doctor repairs it by surgical patching or grafting.
– Coronary Artery Blockage:
Opening up the arteries that supply the heart is the most common type of heart surgery. It involves either coronary artery bypass grafting (CABG) or less drastic procedures such as angioplasty, which may include implanting of a stent.
– Chest Pain:
When the preceding treatments have been unable to relieve the chest pain called angina, a surgeon can use a laser to drill small channels in the heart muscle. This procedure, called myocardial revascularization, seems to improve blood flow within the muscle, thereby relieving pain.
 – Valve Failure:
– Valve Failure:
When a valve in the heart no longer performs adequately, it must be repaired or replaced. This heart surgery traditionally requires opening the patient’s chest and a long recovery time – six weeks to six months. In some cases (including mine) the surgeon can perform the surgery through an incision under one breast. The doctor reaches the heart by pushing apart two ribs. Recovery time from this surgery is weeks rather than months.
– Total Heart Failure:
If all other treatments have failed, the patient may receive a heart transplant. While waiting for a transplant, surgeons may implant a mechanical pump or an artificial heart.
My Lucky Diagnosis
Some heart problems creep up on you. If your family doctor is alert, he or she will ship you to a cardiologist in time to delay the worst symptoms.
Other heart problems are silent. They never appear until you have a heart attack and need to get to a hospital within a few minutes. If you happen to be hiking in Nepal when that happens, well, good luck to you!
My heart problem was somewhere in between. Most men on my father’s side of the family have mitral valve problems, so my cardiologist had been keeping an eye on my valve. The “keeping an eye” required no medication but included office visits every six months.
Visiting Dr John
In October I had one of these routine visits. Of course, I mentioned my current lifestyle symptoms, which at that time were depressed appetite and weight loss. Those symptoms started prior to my prostate surgery but I thought they might be related to that experience.
But Dr John had a hunch. She listened to my heart murmur, a rushing sound caused by valve reflux or regurgitation. She observed that it was much louder than six months before. Noting my current symptoms she suspected an uncommon ailment: endocarditis, specifically an infection of the inner surface of the heart.
Dr John questioned me and determined that I didn’t have any other of the usual symptoms of endocarditis: a fever, recent dental surgery, spots or lumps on the feet or hands, edema and so forth. Nevertheless, she immediately scheduled an echocardiogram to compare against one taken a year previously. When the echo showed increased valve leakage, she instructed me to go to the hospital immediately for a “blood culture.”
When taking a blood culture, multiple blood samples are taken in as antiseptic a manner as possible. They are incubated at body temperature and examined daily for five days, to detect bacterial growth indicating an infection. My blood showed infection after a single day of incubation and my alarmed cardiologist told me to immediately check in to the hospital.
A New Hospital Adventure
My previous surgery, memorialized in a five-part blog, taught me a great deal about the hospital experience. However, that surgery required only a single overnight stay, plus a week of follow-up treatment. In contrast, my heart surgery kept me in the hospital for sixteen nights, including three nights in the intensive care unit. After the hospital released me I would need four more weeks of antibiotic infusions, three-plus months of medications and probably “cardiac rehabilitation.” Compared with my prostate surgery, this was a “big fancy deal.”
Naturally, I checked in to Beaumont Hospital, the local Grosse Pointe hospital where I had my successful prostate surgery six months before.
What I Learned About Hospital Surgery
Things That I Already Knew:
Nurse’s rolling computer to enter patient data
1. When you check into a hospital, you must give up all expectations of privacy or modesty.
2. There is no rest in a hospital. It seems to be routine to monitor and measure everything as long as you’re there. Every four hours day and night the nurse would measure my “vital signs”: blood oxygen saturation, pulse, oral temperature and blood pressure. Several more times during the day a technician would visit to draw my blood.
3. Hospitals have detailed and strict systems. In my case, docs and nurses read records before every visit, and enter records after every visit. So they are well coordinated and communicating. Frequent requests to state name and birthdate verify that data is entered for the correct patient. Portable printers produce labels with name and birthdate which are immediately put on every blood draw tube. Nevertheless, once in a while human error can occur. You just have to hope that it’s a minor, correctable mistake like the misplaced blood draws described later.
4. There are many blood draws – in my case several times a day. This is hard on the veins, because when you overwork a vein with blood draws it blows up. It also blows up if the needle accidentally goes too deep and punctures the back side of the vein.
5. Healthcare facilities are commonly criticized for having lousy food. Nevertheless, I found the food offered by Beaumont Hospital to be excellent. The cardio docs had me on a “heart healthy” diet that barred important food groups as cheese, real butter and fried food. However, the menu still offered a number of food choices that I found tasty. Others may disagree, but I give the Beaumont food services high marks for doing a difficult job very well.
Things That I Newly Learned:
6. Once you are admitted to the hospital, they won’t let you out until every specialist seeing you discharges you. In my case, this meant that both the cardiologist and the infectious disease specialist had to OK my release.
7. Nurses work 12 hour shifts. Their actual time is longer because they have to overlap with the next shift to do the handover. No matter how many days a week they work, that is a tough career path.
8. For some procedures a nurse will say, “you’re going to feel a little pressure now.” In this context “pressure” is a circumlocution for “pain.” The nurse is trained to help the patient re-frame or re-interpret their feelings in a more positive way. Similarly, during one blood draw the tech told me to take a deep breath before she poked me, to distract me from thinking about the needle.
9. Medical professionals provide valuable tools with which you can tell when you are exerting unhealthy effort. For example:
– The physical therapists wanted me to walk several times a day in the hospital. But they said, if I am no longer able to talk smoothly to a companion without catching a breath, I’m overdoing it. It’s time to pause and rest.
– Dr John, my cardiologist, prescribes that I should never exert my muscles so much that I’m making a strained face.
10. Surgery that’s called “minimally invasive” is not “non-invasive” or “imperceptibly invasive.” It’s just less invasive than something else, and that something else might be a major piece of work. In the case of the heart, minimally invasive surgery is still a big deal. I believe that there are no minor heart surgeries, only “big” and “bigger yet.”
Souvenirs
My surgical incisions healed quickly enough, but I noticed a lump under the skin near my groin scar. It was where I expected the repaired femoral artery and vein to reside. I asked a nurse about it and she said: “When you have surgery, it’s reasonable to expect that you will have some souvenirs from the experience.” The lump went away as I healed, but I thought the nurse’s expression was apt.
Here are the souvenirs I still enjoy:
 1. Scars.
1. Scars.
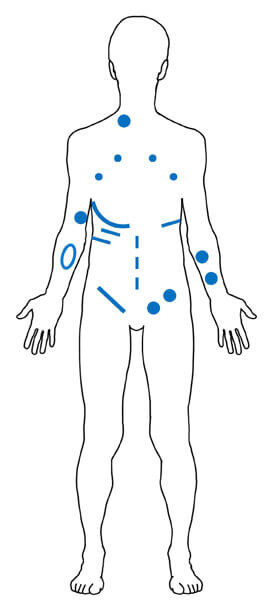
The “minimally invasive” heart surgery required many penetrations of the holy temple of my body. The adjoining sketch shows a G-rated version of the intrusions that punctured my skin:
– The dots are small punctures for catheters, IVs (including PICC line) and temporary pacemaker wires. Those have healed and have mostly disappeared.
– The lines are larger incisions that have left surgical scars. The scars will slowly fade, but probably never disappear. The long one under the right breast was the incision through which the heart surgery was performed. The one in the groin provided access to hook up the heart-lung machine during surgery. The shorter horizontal lines under each breast mark the location of the “chest tubes” that drained fluid from my innards.
– The oval on my right forearm marks the swollen area where my vein “blew up.”
– The vertical dashed line on the belly is the fading scar from my previous prostate surgery.
Rats, there goes my career as a body double!
2. EKG.
After taking an EKG, my cardiologist Dr John made an interesting comment. She said, if another doctor ever takes your EKG, they may ask you, “When did you have your heart attack?” Now I have never had a heart attack. However, any major disturbance of the heart, including heart surgery, apparently changes the heart’s EKG pattern for the rest of your life.
3. Lifestyle Changes.
Life-long adjustments that are detailed in a later installment. These include medical follow-ups and “don’t ever shovel snow again!”
This has been an overview of my heart surgery experience. The next installment of this blog will describe the path that many of us are destined to take. It’s called “What Brings Us to the Operating Room Before Surgery.”
Drawing Credit: Male silhouette adapted from public domain drawing in Wikimedia
Image Credits:
– Heart attack courtesy of Moini on openclipart.org
– Flying Heart courtesy of OIKu on openclipart.org
– Photo of nurse’s computer station by Art Chester
Dear Art,
First I am happy this “adventure” is behind you, without any complications, and not having endured a heart attack.
I am thankful for your warning and explanation of the process some of us may have go through.
I hope you continue to live well and enjoy life,
Metin
Thanks for your good wishes, Metin, which I send to you as well! I feel fortunate that I had symptoms that caught my problems before they surprised me.
First, I’m so happy for your recovery and good spirits. Sad that you had to endure it. But also very thankful for how you share so much that will help and encourage others. Excellent blog, once again! Thank you!
Thank you for your comment, Rick! If it helps readers, that is just the reward I hope for.
Art
I am very happy that you are well and living a healthy lifestyle.
Great blog.
Juan Lam
Thanks, Juan! And many healthy wishes to you as well! My experience reinforces my belief that it’s better to keep close to the docs than to wait until a heart attack strikes and then try to survive it and fix it.
Comment from Dane Jordan (paramedic): Just checking in on you. I read your heart blog. Great information. I wanted to share that the reason for the questioning of when you had a heart attack is because of what they call a “pathological Q wave” in your ECG. The Q wave is the first negative deflection in the QRS section of your heart beat. The first round pump is the “P” wave and indicates the is depolarization of the atria. The QRS is the depolarization ventricle firing. A pathological “Q” wave means it’s a little deeper than 1/3 the height of the R wave, first positive deflection after the Q wave, or it’s wider than 1mm. Both are indicators of a past cardiac event. Looking forward to the rest of the blog.